




Medically Reviewed by Dr. Poobalan A/L Kandasamy
Introduction
If your doctor has recommended either an endoscopy or an OGDS (Oesophago-Gastro-Duodenoscopy) gastroscopy and you are not quite sure what each one involves, or how they differ, you are not alone.
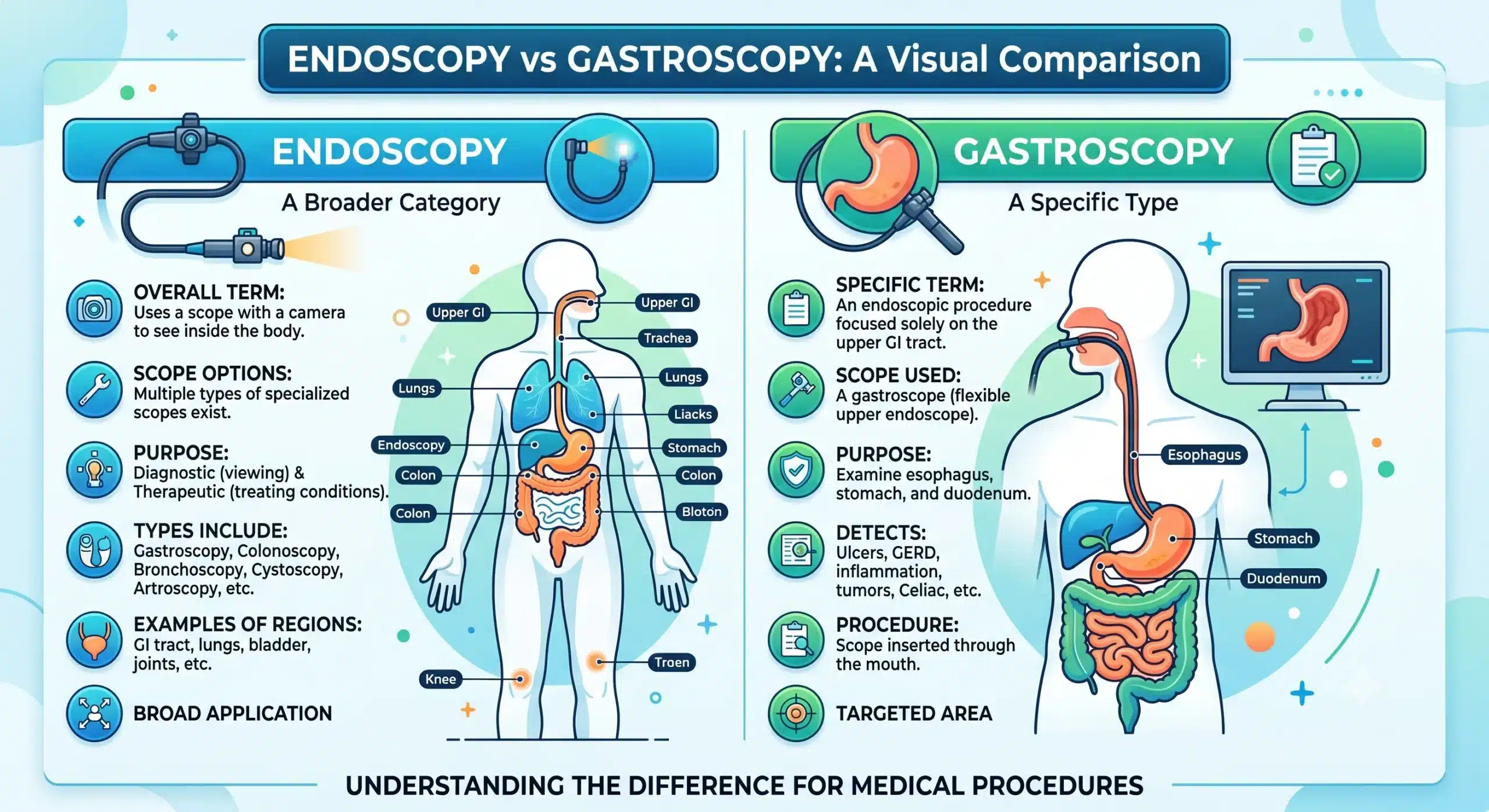
Here is the short version: endoscopy is a broad category of medical procedure that uses a thin, flexible tube fitted with a camera and light to examine the inside of the body without large incisions. Gastroscopy is one specific type of endoscopy, focused exclusively on the upper digestive tract. In other words, every gastroscopy is an endoscopy, but not every endoscopy is a gastroscopy.
The confusion is understandable. In everyday clinical practice, doctors and patients sometimes use the word “endoscopy” informally to mean gastroscopy, particularly when discussing upper gastrointestinal symptoms.
Both procedures are performed by gastroenterologists and both rely on the same fundamental technology. But they are not the same thing, and understanding the difference matters when you are trying to make sense of your own care.
What Is an Endoscopy?
An endoscopy is a minimally invasive procedure that allows doctors to examine organs and tissues inside the body using an endoscope. The word itself comes from the Greek endon (within) and skopein (to look). The endoscope, a long flexible tube with a camera at its tip, transmits live images to a monitor, allowing the physician to inspect the lining of internal structures in real time, collect tissue samples (biopsies), and in some cases perform minor therapeutic procedures, all without the need for open surgery [1].
Endoscopy serves both diagnostic and therapeutic purposes. It is used to identify the source of unexplained symptoms, detect abnormalities such as inflammation, ulcers, polyps, and early-stage cancers, and to deliver treatments such as removing polyps, stopping bleeding, or dilating narrowed passages. The specific type of endoscopy ordered depends entirely on which part of the body needs to be examined.
Types of Endoscopy
Endoscopy is an umbrella term covering a wide range of procedures, each with its own focus and technique. The most commonly performed types include:
-
- Gastroscopy: Also known as upper endoscopy or oesophagogastroduodenoscopy (OGD), this examines the oesophagus, stomach, and duodenum. It is the type most people are thinking of when they say “endoscopy” in the context of digestive complaints.
- Colonoscopy: Examines the large intestine (colon) and rectum. It is the gold standard for colorectal cancer screening and is also used to investigate symptoms such as rectal bleeding, changes in bowel habits, and abdominal pain.
- Bronchoscopy: Examines the airways and lungs via the nose or mouth. It is used to investigate persistent cough, haemoptysis (coughing up blood), unexplained breathlessness, or suspected lung infection or tumour.
- Cystoscopy: Examines the bladder and urinary tract. It is typically recommended for patients with blood in the urine, frequent urinary tract infections, or urinary symptoms that have not responded to treatment.
What Is a Gastroscopy?
Gastroscopy, sometimes written as gastroscopy or OGD (oesophagogastroduodenoscopy), is a procedure in which a gastroscope, a specialised flexible tube with a camera and light, is gently inserted through the mouth and guided down the throat, through the oesophagus, and into the stomach and duodenum. The physician views the lining of these structures on a monitor in real time.
The three organs examined during a gastroscopy are the oesophagus (the tube connecting the throat to the stomach), the stomach itself, and the duodenum (the first and shortest section of the small intestine, which receives partially digested food from the stomach). This makes gastroscopy the procedure of choice for investigating symptoms originating in the upper gastrointestinal tract.
Doctors typically recommend a gastroscopy when a patient presents with persistent heartburn or acid reflux, difficulty swallowing, unexplained upper abdominal pain, nausea or vomiting that does not resolve, unexplained weight loss, or signs of upper gastrointestinal bleeding such as dark or tarry stools. It is also used to take biopsies, check for the bacteria Helicobacter pylori, and treat certain conditions such as bleeding ulcers on the spot.
So are endoscopy and gastroscopy the same thing? Not exactly. Gastroscopy is a specific, clearly defined subtype of endoscopy. When a gastroenterologist says they are sending you for a “gastroscopy” or an “upper endoscopy,” they mean the same procedure [1]. When they say “endoscopy” without further context, they are likely using the term informally to mean gastroscopy, though technically the word covers a much wider range of procedures.
Difference Between Endoscopy and Gastroscopy
The table below sets out the key differences side by side.
| Endoscopy (General) | Gastroscopy | |
|---|---|---|
| Purpose | Diagnostic and therapeutic examination of various internal organs and body structures | Diagnosis and treatment of upper gastrointestinal tract conditions |
| Organs Examined | Varies by type: GI tract, airways, bladder, joints, abdominal cavity, and more | Oesophagus, stomach, and duodenum, the first part of the small intestine |
| Procedure Method | Endoscope inserted through natural openings or small incisions depending on the target area | Endoscope inserted through the mouth and guided down the throat |
| Duration | Varies from 15 minutes to over an hour depending on the type and complexity | Typically 15 to 30 minutes |
| Preparation | Varies by procedure type, such as fasting, bowel prep, or other specific requirements | Fasting for 6 to 8 hours before the procedure, with medication review as advised |
| Anaesthesia | Sedation or general anaesthesia depending on the procedure type | Light sedation or local throat anaesthetic spray, with sedation available on request |
When Do You Need an Endoscopy or Gastroscopy?
Both procedures are typically recommended when symptoms point to a problem in the gastrointestinal tract that cannot be adequately assessed through physical examination, blood tests, or imaging alone. Some of the most common reasons a gastroenterologist might recommend one include:
-
- Persistent or worsening stomach pain that has not responded to standard treatment
- Frequent acid reflux or heartburn, particularly if it is not controlled by medication
- Difficulty swallowing (dysphagia), which may indicate narrowing or obstruction in the oesophagus
- Unexplained gastrointestinal bleeding, including blood in the stool or vomiting blood
- Chronic nausea or vomiting without a clear cause
- Unintentional weight loss, which can be a red flag for malignancy or malabsorption
- Suspected peptic ulcers, gastritis, or Helicobacter pylori infection
Warning Signs That Require Immediate Medical Attention
Certain symptoms should not be managed with a wait-and-see approach. Seek urgent medical attention if you experience any of the following:
-
- Vomiting blood or material that looks like coffee grounds
- Black, tarry, or maroon stools, which may indicate significant internal bleeding
- Sudden, severe abdominal pain
- Difficulty breathing alongside upper GI symptoms
- Rapid, unexplained weight loss combined with difficulty swallowing
These symptoms may require emergency endoscopy rather than an elective procedure, and time matters in these situations.
How to Prepare for Endoscopy and Gastroscopy
Preparation varies depending on the type of procedure, but for a gastroscopy, the requirements are relatively straightforward [1]:
-
- Fasting: You will typically be asked to fast for at least six to eight hours before the procedure. This means no food and no drinks other than small sips of water (unless instructed otherwise). An empty stomach allows for clearer images and reduces the risk of aspiration.
- Medication adjustments: Inform your doctor about all medications you are currently taking. Blood-thinning medications such as warfarin, aspirin, or clopidogrel may need to be paused before the procedure. Diabetic patients will receive specific instructions about insulin or oral hypoglycaemic agents.
- What to wear and bring: Wear comfortable, loose-fitting clothing. Leave jewellery and valuables at home. If you are receiving sedation, you will need a responsible adult to drive you home and stay with you for the rest of the day.
- Follow your doctor’s instructions: Your gastroenterologist or the procedure unit will provide you with a pre-procedure information sheet. Read it carefully and ask questions if anything is unclear.
What Happens During the Procedure?
A gastroscopy typically follows this sequence [1]:
- You will be asked to remove any dentures and lie on your left side on the procedure table.
- A local anaesthetic throat spray is applied to numb the back of your throat. If you have requested sedation, a cannula will be placed in your arm and the sedative administered.
- A mouthguard is placed between your teeth to protect both you and the endoscope.
- The gastroscope is gently guided through your mouth, down the oesophagus, and into the stomach and duodenum. Air is introduced to gently inflate the stomach so the camera can see clearly. This may cause some bloating or belching.
- The physician inspects the lining of the oesophagus, stomach, and duodenum. If anything requires closer examination, small biopsy samples can be taken using instruments passed through a channel in the endoscope. Biopsies are painless.
- Once the examination is complete, the endoscope is slowly and carefully withdrawn. The entire procedure is viewed on a monitor by the physician throughout.
How Long Does the Procedure Take?
A diagnostic gastroscopy typically takes between 15 and 30 minutes from start to finish [1]. If additional steps are required, such as biopsies, removal of polyps, or treatment of a bleeding vessel, the procedure may take a little longer. After the procedure, you will be monitored in a recovery area for 30 to 60 minutes until the sedative has worn off.
Is Gastroscopy or Endoscopy Painful?
Most patients describe gastroscopy as uncomfortable rather than painful. The throat spray numbs the gag reflex, which makes passage of the scope more tolerable. Sedation, when used, helps most patients feel relaxed and drowsy, and many do not remember the procedure at all. Some people experience a mild sore throat or bloating in the hours after the procedure; both typically resolve within a day [3].
Risks and Benefits
The benefits of gastroscopy and endoscopy generally far outweigh the risks for the vast majority of patients.
-
- Benefits of early diagnosis: Endoscopy allows conditions to be identified and sometimes treated in a single procedure, often before they become serious. Early detection of precancerous changes, ulcers, or infections can significantly alter the course of treatment and outcomes.
- Risks: Serious complications from diagnostic gastroscopy are rare. The most frequently cited risks include minor bleeding at the biopsy site (usually self-limiting), a small risk of infection, and reactions to sedation. Perforation of the GI tract is a rare but serious complication.
- Overall safety: Endoscopy is a well-established, widely performed procedure with a strong safety record. Major complications occur in fewer than 2% of cases, and the procedure is considerably safer than open surgery for diagnostic purposes.
Research consistently supports the safety profile of both procedures when performed by trained endoscopists in appropriately equipped settings [2] [4] [5].
Recovery After Endoscopy or Gastroscopy
Recovery from a gastroscopy is typically quick. Most patients are observed in a recovery area for 30 to 60 minutes after the procedure and are discharged the same day.
-
- Recovery time: If you received sedation, you should not drive, operate machinery, sign legal documents, or make important decisions for at least 24 hours.
- Eating after the procedure: Most patients can eat and drink normally once the throat numbness has worn off, usually within an hour or two. Start with soft, light foods if your throat feels tender.
- When to call your doctor: Contact your healthcare team if you experience significant pain, persistent vomiting, fever, difficulty swallowing, or any signs of bleeding such as dark stools or vomiting blood in the days following the procedure.
FAQs
Is endoscopy painful?
For most people, endoscopy causes discomfort rather than pain. The combination of a local throat spray and optional sedation means most patients tolerate the procedure well. A mild sore throat or bloating in the hours afterwards is common but short-lived.
What to eat after endoscopy?
Once the throat anaesthetic has worn off, usually within one to two hours, you can return to eating normally. Soft foods like yoghurt, soup, or toast are a gentle starting point if your throat feels tender. Avoid very hot drinks for the rest of the day. Your care team will give you specific instructions if biopsies were taken or any treatment was performed during the procedure.
Can gastroscopy detect drug traces in the body?
No. Gastroscopy is a visual examination of the upper digestive tract lining. It cannot detect drugs, medications, or substances in the bloodstream. If drug detection is required for medical or legal purposes, blood or urine testing is the appropriate method. Gastroscopy is designed to diagnose structural and mucosal abnormalities in the oesophagus, stomach, and duodenum [1].
When to Consult a Gastroenterologist
Early diagnosis is one of the most powerful tools in digestive health. Many serious conditions, including gastric cancer, Barrett’s oesophagus, and peptic ulcer disease, are far more manageable when caught early. Endoscopy and gastroscopy make that early detection possible.
If you have been experiencing persistent upper GI symptoms, have a family history of gastrointestinal conditions, or have been referred by your GP, do not delay in seeking specialist advice. A gastroenterologist will review your history, discuss whether an endoscopy or gastroscopy is appropriate, and explain what to expect at every step.
At ACC, our gastroenterology team provides comprehensive assessment and endoscopic services in a supportive, patient-focused environment.
References
[1] Ehsan, M. and Iqbal, P. (2025) ‘Esophagogastroduodenoscopy’, in StatPearls. Treasure Island (FL): StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK532268/
[2] Green, J. et al. (2022) ‘Complications of diagnostic upper gastrointestinal endoscopy: common and rare – recognition, assessment and management’, Frontline Gastroenterology, 14(1), pp. 48–56. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC9806027/
[3] Goudra, B. et al. (2021) ‘Sedation practices for routine gastrointestinal endoscopy: a systematic review of recommendations’, BMC Gastroenterology, 21(1), p. 5. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC7792218/
[4] Goyal, H. et al. (2022) ‘Gastrointestinal endoscopy-associated infections: update on an emerging issue’, Annals of Medicine, 54(1), pp. 1003–1014. Available at: https://pubmed.ncbi.nlm.nih.gov/35262904/
[5] American Society for Gastrointestinal Endoscopy (ASGE) Standards of Practice Committee (2012) ‘Adverse events of upper GI endoscopy’, Gastrointestinal Endoscopy, 76(4), pp. 707–718. Available at: https://www.asge.org/docs/default-source/education/practice_guidelines/doc-adverse-events-of-upper-gi-endoscopy.pdf









